

Introduction
Patients with relapsed/refractory (R/R) diffuse large B-cell lymphoma (DLBCL) who are not eligible for autologous stem cell transplant (ASCT) have a poor prognosis. Tafasitamab (MOR208) is an Fc-enhanced, humanized, monoclonal antibody that targets CD19, which is broadly expressed across B-cell malignancies, including DLBCL. The immunomodulatory drug lenalidomide (LEN) has antiproliferative and antiangiogenic effects.
L-MIND (NCT02399085) is an ongoing, open-label, single-arm, Phase II study of tafasitamab + LEN in patients with R/R DLBCL who are ineligible for ASCT. L-MIND results from prespecified patient subgroup analyses were presented previously (primary analysis: data cut-off Nov 30, 2018). Here, we report long-term clinical efficacy from the L-MIND study after a median follow-up of 31.8 months for overall survival (OS) (data cut-off: Nov 30, 2019).
Methods
Patients enrolled were aged ≥18 years with R/R DLBCL (1-3 prior systemic therapies, including ≥1 CD20-targeting regimen), ASCT-ineligible and with an Eastern Cooperative Oncology Group performance status of 0-2.
Patients received 28-day cycles of tafasitamab (12 mg/kg intravenously), once weekly during Cycles 1-3 with a loading dose on Cycle 1 Day 4, then every 2 weeks during Cycles 4-12. LEN (25 mg orally) was administered on Days 1-21 of Cycles 1-12. After Cycle 12, progression-free patients received tafasitamab every 2 weeks until disease progression.
The primary endpoint is objective response rate (ORR; partial response [PR] + complete response [CR]), assessed centrally by an independent review committee. Secondary endpoints include duration of response (DOR), progression-free survival (PFS), OS and safety analyses.
Results
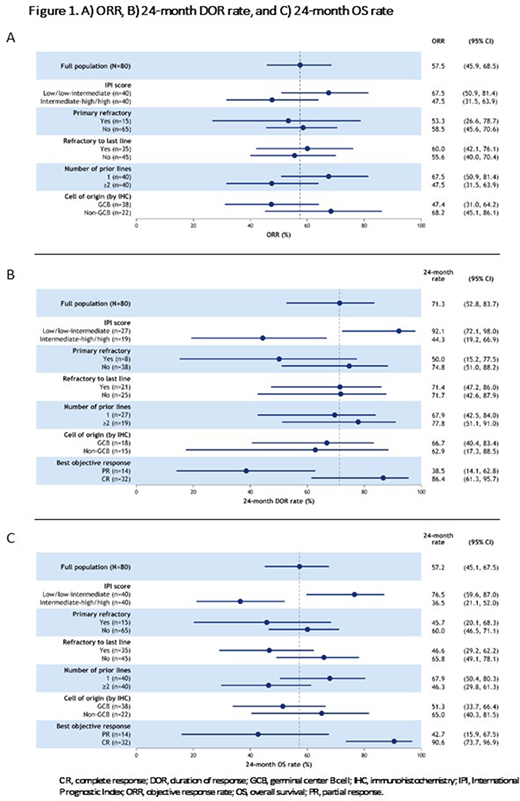
Of 81 patients enrolled, 80 patients received tafasitamab + LEN and were included in the full analysis set (FAS) for efficacy. Median follow-up was 22.7 months. In the FAS, ORR was 57.5% (95% confidence interval [CI]: 45.9-68.5) (Figure 1A). The CR rate was 40.0% (n=32/80), of which 90.6% (n=29/32) were PET-confirmed. Median time to response (PR or CR) was 2.0 months and median time to CR was 6.1 months. Median DOR was 34.6 months (95% CI: 26.1-34.6); median PFS was 12.1 months (95% CI: 6.3-not reached [NR]); and median OS was 31.6 months (95% CI: 18.3-NR). The 24-month DOR and OS rates were 71.3% (95% CI: 52.8-83.7) (Figure 1B) and 57.2% (95% CI: 45.1-67.5) (Figure 1C), respectively.
In the subgroup analysis, patients with CR as best objective response had better outcomes than those with PR: median DOR, NR (95% CI: 26.1-NR) vs 5.6 months (95% CI: 2.2-34.6); 24-month DOR rate, 86.4% (95% CI: 61.3-95.7) vs 38.5% (95% CI: 14.1-62.8); and 24-month OS rate, 90.6% vs 42.7%.
Patients with 1 prior line of therapy had a trend for better outcomes than those with ≥2 prior lines: ORR, 67.5% vs 47.5%; 24-month OS rate, 67.9% vs 46.3%. The 24-month DOR rate was similar by the number of prior lines (1 prior line: 67.9% [95% CI: 42.5-84.0] vs ≥2 prior lines: 77.8% [95% CI: 51.1-91.0]).
ORR was similar by primary refractory vs non-primary refractory status (53.3% vs 58.5%); however, primary refractory status impacted 24-month DOR (50.0% vs 74.8%, respectively). Patients refractory to their last line of therapy achieved similar ORRs to those who were not (60.0% vs 55.6%). The 24-month DOR was similar regardless of refractory status to last therapy (Figure 1B), and 24-month OS rates were higher in non-refractory patients (Figure 1C).
As expected, patients with a low/low-intermediate International Prognostic Index score had better outcomes than those with an intermediate-high/high score: ORR, 67.5% vs 47.5%; 24-month DOR rate, 92.1% vs 44.3%; and 24-month OS rate, 76.5% vs 36.5%.
Based on the Hans algorithm, outcomes were encouraging independent of germinal center B-cell (GCB) DLBCL (n=38) or non-GCB DLBCL (n=22) disease: ORR, 47.4% vs 68.2%; median DOR, 34.6 vs 26.1 months; 24-month DOR rate, 66.7% vs 62.9%; and 24-month OS rate, 51.3% vs 65.0%.
Conclusions
Long-term L-MIND subgroup data show that encouraging activity observed at primary analysis remains durable after ≥2 years of follow-up; patients with CR continue to experience long DOR and high OS. Although the influence of poor prognosis risk factors is still evident, the clinical activity of tafasitamab in combination with LEN followed by tafasitamab monotherapy continues to show promise in difficult-to-treat ASCT-ineligible patients with R/R DLBCL.
Maddocks:Pharmacyclics: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Karyopharm: Consultancy; ADC Therapeutics, AstraZeneca: Consultancy; BMS: Consultancy, Research Funding; Morphosys: Consultancy, Honoraria; Celgene: Consultancy, Honoraria. Duell:Morphosys: Research Funding. González-Barca:Sandoz: Consultancy; Gilead: Consultancy; Janssen: Consultancy, Honoraria; Abbvie: Honoraria; Takeda: Honoraria; Roche: Honoraria; MorphoSys: Other; Celtrion: Consultancy; Kiowa: Consultancy; Celgene: Consultancy. Jurczak:Janssen, MeiPharma, Merck, Pharmacyclics, Roche, Tekeda, TG Therapeutics: Research Funding; Jagiellonian University: Ended employment in the past 24 months, Research Funding; Maria Sklodowska-Curie National Research Institute of Oncology: Consultancy, Current Employment. Liberati:Novartis: Research Funding; GSK: Research Funding; Incyte: Honoraria; Janssen: Honoraria, Research Funding; Oncopeptides: Research Funding; Morphosys: Research Funding; Karyopharm: Research Funding; Pfizer: Research Funding; Takeda: Research Funding; Roche: Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Honoraria, Research Funding; Onconova: Research Funding; Verastem: Research Funding. de Vos:Bayer: Consultancy; Verastem: Consultancy. Nagy:MorphoSys AG: Patents & Royalties. Obr:Roche: Honoraria. Gaidano:Sunesys: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astrazeneca: Membership on an entity's Board of Directors or advisory committees. Abrisqueta:Roche: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Speakers Bureau; AbbVie: Consultancy, Honoraria, Speakers Bureau. André:Celgene: Other, Research Funding; Johnson & Johnson: Research Funding; Amgen: Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Roche: Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Abbvie: Consultancy; Seattle Genetics: Consultancy; Novartis: Consultancy, Research Funding; Gilead: Consultancy, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Bristol-Myers-Squibb: Consultancy, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Karyopharm: Consultancy; Takeda: Consultancy; CHU UCL Namur, site Godinne, Yvoir, Belgium: Current Employment. Dreyling:Celgene: Consultancy, Research Funding, Speakers Bureau; Roche: Consultancy, Research Funding, Speakers Bureau; Novartis: Consultancy; Janssen: Consultancy, Research Funding, Speakers Bureau; Abbvie: Research Funding; Astra Zeneca: Consultancy; Beigene: Consultancy; Gilead: Consultancy, Research Funding, Speakers Bureau; Bayer: Consultancy, Speakers Bureau. Menne:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Kite/Gilead: Honoraria, Speakers Bureau; Novartis: Honoraria, Other: Travel costs, Speakers Bureau; Pfizer: Honoraria, Other: Travel costs, Speakers Bureau; Celgene: Honoraria, Other: Travel grants; Roche: Speakers Bureau; Janssen: Honoraria, Research Funding, Speakers Bureau; Astra Zeneca: Research Funding; Takeda: Honoraria, Speakers Bureau. Dirnberger-Hertweck:MorphoSys AG: Current Employment. Weirather:MorphoSys AG: Current Employment. Ambarkhane:MorphoSys AG: Current Employment. Salles:Takeda: Honoraria; BMS/Celgene: Honoraria, Other: consultancy or advisory role; Autolos: Other: consultancy or advisory role; Abbvie: Other: consultancy or advisory role; Roche: Honoraria, Other: consultancy or advisory role; Novartis: Honoraria, Other: consultancy or advisory role; MorphoSys: Honoraria, Other: consultancy or advisory role; Janssen: Honoraria, Other: consultancy or advisory role; Epizyme: Honoraria, Other: consultancy or advisory role; Kite, a Gilead Company: Honoraria, Other: consultancy or advisory role ; Debiopharm: Consultancy, Honoraria, Other: consultancy or advisory role; Genmab: Honoraria, Other; Karyopharm: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal